A 36 year old soldier developed a flu-like illness (fever, chills, headache, myalgia) 4 days after returning to Jakarta, Indonesia, from a 1 year posting to Papua New Guinea. He was known to have chronic hepatitis B infection, with chronically mildly abnormal liver function tests, but was not on any treatment for this, and had otherwise been well. 3 days later he developed nausea and vomiting and abdominal pain, and jaundice was noted. After a week of this illness he was admitted to hospital where he was thought to have obstructive jaundice, so on the 10th day of his illness he was transferred to a tertiary centre.
Case contributed by Dr Jonny and colleagues from Jakarta, Indonesia. From the UK Kidney Association’s international case presentation series.

Papua New Guinea. CC-BY; credits at foot of page
On transfer he was initially alert, deeply jaundiced, apyrexial, BP 107/53, but becoming obtunded. Some upper abdominal tenderness was noted. Ultrasound showed normal liver oultline no obstruction, thickened gallbladder wall with sludge. Elastography suggested severe liver fibrosis. Blood test results are shown (click to enlarge).
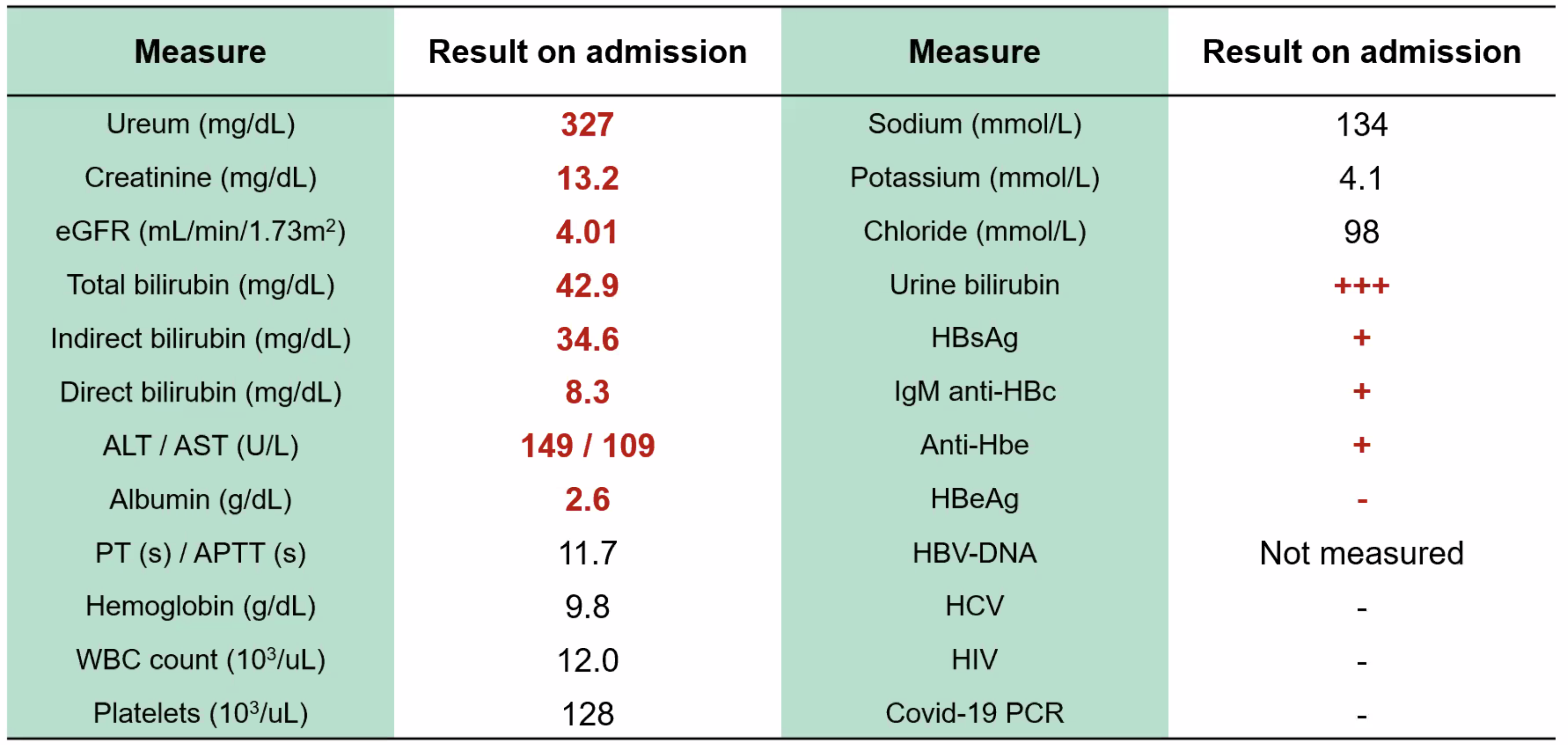 The urea converts to 117 mmol/l, Creat 1160 micromol/l. High enough for uraemic encephalopathy. He was also oliguric. He was anaemic, Hb 7.6 g/dl, wbc 19.9 (neutrophilia), plats 462.
The urea converts to 117 mmol/l, Creat 1160 micromol/l. High enough for uraemic encephalopathy. He was also oliguric. He was anaemic, Hb 7.6 g/dl, wbc 19.9 (neutrophilia), plats 462.
The initial suspicion was that he had an acute exacerbation of chronic HBV hepatitis, possibly with acute cholecystitis, complicated by AKI.
Questions
- Do you agree? What other conditions would you want to rule out?
- Suggest up to three investigations to rule in or out your key differentials.
CDC
Last Updated on February 2, 2025 by admin